
Why Multi-Cancer Early Detection Is Becoming Part of Routine Care
Why Multi-Cancer Early Detection Is Becoming Part of Routine Care
Why Multi-Cancer Early Detection Is Becoming Part of Routine Care
Multi-cancer early detection tests are changing what's possible — and what's expected of preventive care.
Multi-cancer early detection tests are changing what's possible — and what's expected of preventive care.
Longevity Science
Longevity Science
Published:
Published:
April 29, 2026
April 29, 2026
By Dr. Jeffrey Chen, Medical Director, Peak Health
It was the middle of COVID. I’d just finished intubating my 4th patient that shift. I stepped into the hallway — the only space left in the emergency department — and told a woman in her early fifties that her abdominal pain was due to what appeared to be metastatic ovarian cancer.
She had no prior screening for it. There is no standard screening for it. By the time ovarian cancer causes symptoms — bloating, pelvic pain, feeling full too quickly — it has usually already spread. Her cancer had.
That conversation in the hallway, while ventilators alarmed behind me, highlighted to me that so many of them were avoidable.
The cancers we’re not looking for
Standard care screens for five cancers: breast, cervical, colorectal, lung, and prostate. Those screenings save lives, and they should remain the foundation of any cancer prevention strategy. But nearly 70% of cancer deaths come from types that have no recommended screening test, such as:
Pancreatic
Ovarian
Liver
Esophageal
Gastric
For these cancers, the standard of care has essentially been to wait for symptoms. And by the time symptoms appear, the disease is often advanced.
This isn’t a failure of oncology. Cancer treatment has improved enormously. It’s a failure of detection — a blind spot in how we practice preventive medicine.
What multi-cancer early detection actually does
Multi-cancer early detection (MCED) tests analyze cell-free DNA in the bloodstream — fragments shed by cancer cells that carry distinct chemical signatures called methylation patterns. Those patterns can indicate not just whether a cancer signal is present, but where in the body it’s likely originating. One blood draw. No imaging. No invasive procedure.
The Galleri® test, developed by GRAIL®, is the most clinically validated MCED test currently available. I’ve followed this technology closely for years. It’s one of the reasons I made the transition from emergency medicine into longevity care — the idea that we could screen for dozens of cancer types from a single blood draw felt like the kind of paradigm shift worth building a practice around.
The evidence is substantial. In GRAIL’s PATHFINDER 2 study of nearly 25,000 patients, adding Galleri to standard recommended screenings for breast, cervical, colorectal, and lung cancer detection more than sevenfold. Over half of the cancers detected were caught at stage I or II, when treatment is most effective. And when a cancer signal was detected, the test accurately identified the tissue of origin 92% of the time — giving the physician a clear starting point for diagnostic workup.
(Source: Galleri® for Healthcare Providers).
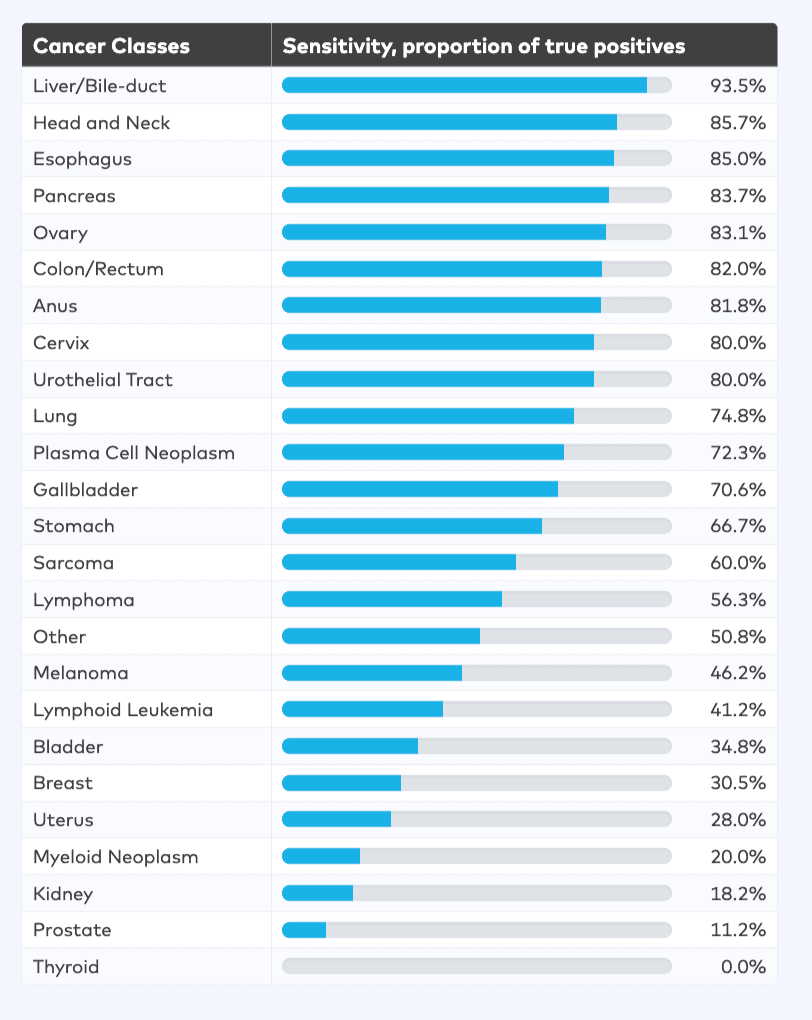
And it happens that those cancers above are what GRAIL are best at detecting.
Who should consider this test
The Galleri test is recommended for adults with elevated cancer risk — generally those 50 or older, or anyone with significant family history or other known risk factors. It requires a prescription and should be used alongside existing recommended screenings, not instead of them.
As a physician, the question I’m really asking is: what does your complete risk picture look like? Family history, inflammatory markers, metabolic health, lifestyle factors — all of it informs whether proactive cancer screening should be part of your care plan. A detected cancer signal is not a diagnosis. It’s clinical information that requires interpretation, follow-up imaging, specialist referral, and context. What happens next depends on everything else we know about you.
Why the clinical relationship matters as much as the test
This is the part I want people to understand: the test is not the intervention. The intervention is what happens after.
A cancer signal detected result sets off a clinical process — imaging, specialist referrals, additional testing — that goes significantly better when a physician who already knows your full health picture is coordinating it. The difference between a cancer signal detected result in the context of a longitudinal care relationship and one received as an isolated data point is enormous. One leads to a clear, guided next step. The other leads to anxiety and fragmented follow-up.
At Peak Health, the Galleri test is now available to eligible members through their existing care relationship. Your physician orders it, reviews the result alongside your complete biomarker history, and guides next steps directly. It’s not a standalone product. It’s part of a comprehensive approach to finding things early, when we can do something about them.
An important note: Galleri is not a crystal ball. It doesn’t replace mammography, colonoscopy, or the screening tests we already know save lives. But for cancers where we currently have nothing — where I’ve had to walk into hallways and deliver the kind of news that opens this piece — it’s the first tool I’ve seen that changes the shape of the problem.
The future of cancer screening
Multi-cancer early detection is moving from cutting-edge to clinical standard. Major health systems are integrating it. The evidence base continues to grow. I believe MCED will become as routine as annual bloodwork or a mammogram within the next decade.
I think about that woman in the hallway often. I think about whether a blood test, drawn six months earlier by a physician who knew her family history and was watching for exactly this kind of risk, might have caught it at stage I instead of stage IV. I can’t go back and change that outcome. But I can build a practice where that conversation happens less often.
If you’re 50 or older, or have elevated cancer risk, it’s worth a conversation with your physician. The goal is never to create anxiety. The goal is to find things early, when they’re still treatable.
Ready to take a proactive approach to your health?
Peak Health brings together elite longevity physicians, 350+ biological data points, and advanced testing — including access to the Galleri multi-cancer early detection test — into one complete care relationship. If you're ready to stop waiting for something to go wrong and start getting ahead of it, schedule a free longevity consult.
The Galleri test is recommended for adults with elevated cancer risk, such as those 50 or older. It does not detect a signal for all cancers, and false positive or false negative results can occur. The Galleri test should be used in addition to routine cancer screenings recommended by your healthcare provider. The Galleri test has not been cleared or approved by the FDA. Rx only.
By Dr. Jeffrey Chen, Medical Director, Peak Health
It was the middle of COVID. I’d just finished intubating my 4th patient that shift. I stepped into the hallway — the only space left in the emergency department — and told a woman in her early fifties that her abdominal pain was due to what appeared to be metastatic ovarian cancer.
She had no prior screening for it. There is no standard screening for it. By the time ovarian cancer causes symptoms — bloating, pelvic pain, feeling full too quickly — it has usually already spread. Her cancer had.
That conversation in the hallway, while ventilators alarmed behind me, highlighted to me that so many of them were avoidable.
The cancers we’re not looking for
Standard care screens for five cancers: breast, cervical, colorectal, lung, and prostate. Those screenings save lives, and they should remain the foundation of any cancer prevention strategy. But nearly 70% of cancer deaths come from types that have no recommended screening test, such as:
Pancreatic
Ovarian
Liver
Esophageal
Gastric
For these cancers, the standard of care has essentially been to wait for symptoms. And by the time symptoms appear, the disease is often advanced.
This isn’t a failure of oncology. Cancer treatment has improved enormously. It’s a failure of detection — a blind spot in how we practice preventive medicine.
What multi-cancer early detection actually does
Multi-cancer early detection (MCED) tests analyze cell-free DNA in the bloodstream — fragments shed by cancer cells that carry distinct chemical signatures called methylation patterns. Those patterns can indicate not just whether a cancer signal is present, but where in the body it’s likely originating. One blood draw. No imaging. No invasive procedure.
The Galleri® test, developed by GRAIL®, is the most clinically validated MCED test currently available. I’ve followed this technology closely for years. It’s one of the reasons I made the transition from emergency medicine into longevity care — the idea that we could screen for dozens of cancer types from a single blood draw felt like the kind of paradigm shift worth building a practice around.
The evidence is substantial. In GRAIL’s PATHFINDER 2 study of nearly 25,000 patients, adding Galleri to standard recommended screenings for breast, cervical, colorectal, and lung cancer detection more than sevenfold. Over half of the cancers detected were caught at stage I or II, when treatment is most effective. And when a cancer signal was detected, the test accurately identified the tissue of origin 92% of the time — giving the physician a clear starting point for diagnostic workup.
(Source: Galleri® for Healthcare Providers).
And it happens that those cancers above are what GRAIL are best at detecting.
Who should consider this test
The Galleri test is recommended for adults with elevated cancer risk — generally those 50 or older, or anyone with significant family history or other known risk factors. It requires a prescription and should be used alongside existing recommended screenings, not instead of them.
As a physician, the question I’m really asking is: what does your complete risk picture look like? Family history, inflammatory markers, metabolic health, lifestyle factors — all of it informs whether proactive cancer screening should be part of your care plan. A detected cancer signal is not a diagnosis. It’s clinical information that requires interpretation, follow-up imaging, specialist referral, and context. What happens next depends on everything else we know about you.
Why the clinical relationship matters as much as the test
This is the part I want people to understand: the test is not the intervention. The intervention is what happens after.
A cancer signal detected result sets off a clinical process — imaging, specialist referrals, additional testing — that goes significantly better when a physician who already knows your full health picture is coordinating it. The difference between a cancer signal detected result in the context of a longitudinal care relationship and one received as an isolated data point is enormous. One leads to a clear, guided next step. The other leads to anxiety and fragmented follow-up.
At Peak Health, the Galleri test is now available to eligible members through their existing care relationship. Your physician orders it, reviews the result alongside your complete biomarker history, and guides next steps directly. It’s not a standalone product. It’s part of a comprehensive approach to finding things early, when we can do something about them.
An important note: Galleri is not a crystal ball. It doesn’t replace mammography, colonoscopy, or the screening tests we already know save lives. But for cancers where we currently have nothing — where I’ve had to walk into hallways and deliver the kind of news that opens this piece — it’s the first tool I’ve seen that changes the shape of the problem.
The future of cancer screening
Multi-cancer early detection is moving from cutting-edge to clinical standard. Major health systems are integrating it. The evidence base continues to grow. I believe MCED will become as routine as annual bloodwork or a mammogram within the next decade.
I think about that woman in the hallway often. I think about whether a blood test, drawn six months earlier by a physician who knew her family history and was watching for exactly this kind of risk, might have caught it at stage I instead of stage IV. I can’t go back and change that outcome. But I can build a practice where that conversation happens less often.
If you’re 50 or older, or have elevated cancer risk, it’s worth a conversation with your physician. The goal is never to create anxiety. The goal is to find things early, when they’re still treatable.
Ready to take a proactive approach to your health?
Peak Health brings together elite longevity physicians, 350+ biological data points, and advanced testing — including access to the Galleri multi-cancer early detection test — into one complete care relationship. If you're ready to stop waiting for something to go wrong and start getting ahead of it, schedule a free longevity consult.
The Galleri test is recommended for adults with elevated cancer risk, such as those 50 or older. It does not detect a signal for all cancers, and false positive or false negative results can occur. The Galleri test should be used in addition to routine cancer screenings recommended by your healthcare provider. The Galleri test has not been cleared or approved by the FDA. Rx only.

Dr. Jeffrey Chen
Dr. Jeffrey Chen
Medical Director
Medical Director
More insights for you.
More insights
for you.
More insights for you.
Explore more reflections, guidance, and practical tools to support your growth and well-being.
Explore more reflections, guidance, and practical tools to support your growth and well-being.

Early Signs of Perimenopause Most Women (and Their Doctors) Miss
Perimenopause often starts years before anyone expects it — and its earliest symptoms are easy to miss. Here's how to recognize them, and why catching them early changes everything.
Published:
Thursday, May 14, 2026

What Is Longevity Medicine and How Does It Work?
A guide to what longevity medicine actually is, how it differs from conventional healthcare, and what it looks like in practice at Peak Health.
Published:
February 28, 2026